the pathogen or protein products. Many secreted
products of b-hemolytic streptococci, for instance,
stimulate antibody responses. Anti-streptolysin O
and anti-DNase B are used as markers of recent
streptococcal infection in the evaluation of Syden-
ham’s chorea and poststreptococcal glomeru-
lonephritis, respectively. Antibodies against struc-
tural proteins are used in the evaluation of hepatitis
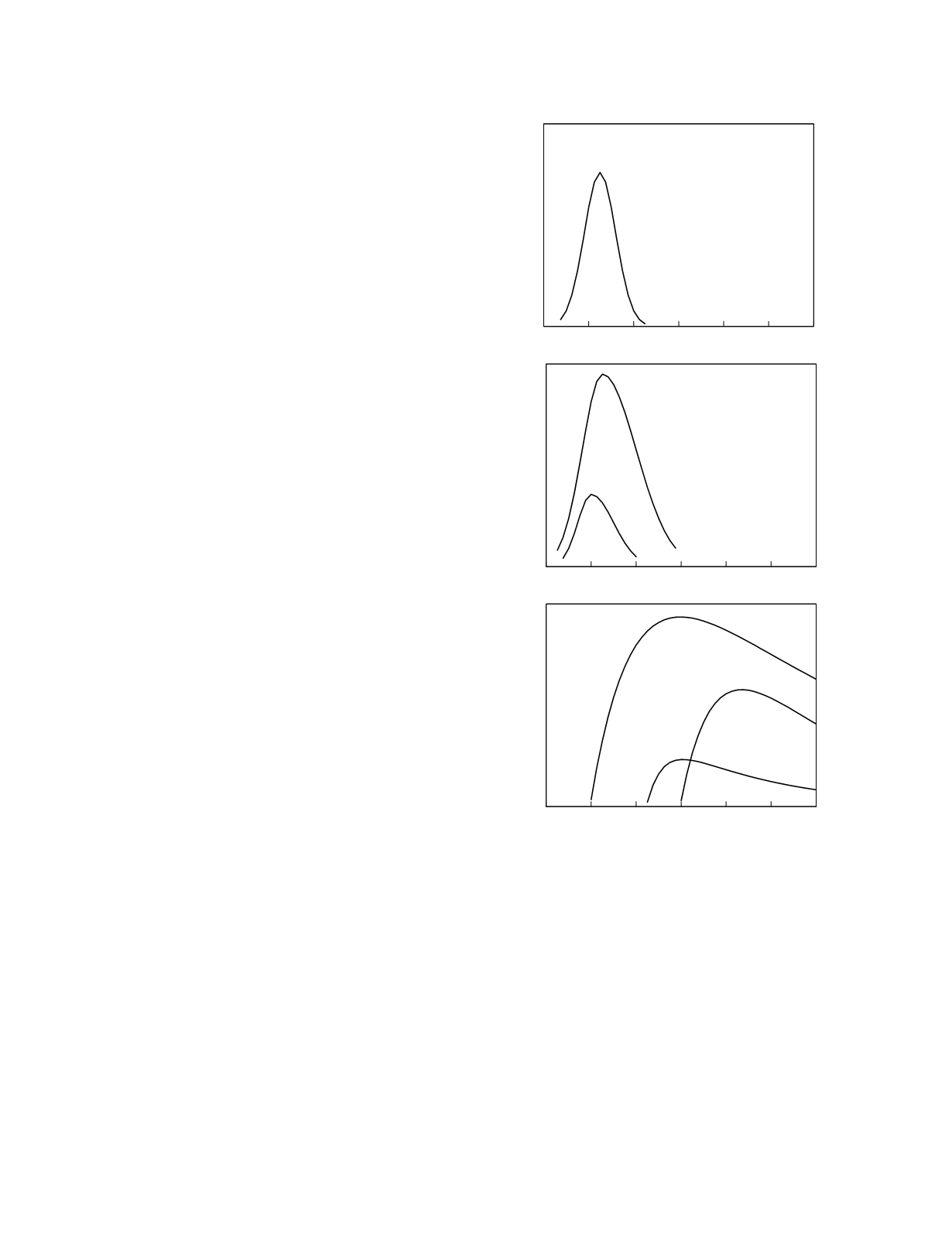
B. The presence of anti-HBc of the IgM class can
be used to distinguish acute from chronic hepatitis in
patients who are HBsAg positive and who have an
ambiguous history. Because anti-HBc first appears
weeks after HBsAg is detectable (Figure 9.4), false
negative results are possible early in the course of
the disease. Anti-HBc of the IgG class is found in
acute and chronic hepatitis. The appearance of anti-
HBe, and the concomitant disappearance of HBeAg,
signals beginning resolution of the disease and is
associated with a low viral replication rate and low
infectivity. The appearance of anti-HBs indicates
recovery from the infection.
Methods in current use for the measurement of
antibodies to pathogens include particle aggluti-
nation, indirect immunofluorescence microscopy,
and various forms of immunoassay. Specificity for
IgM or IgG class test antibodies can be incorporated
into studies that employ a signal-generating reagent
antibody by using an antibody that is immunoglobin
class-specific.
In vitro
antimicrobial susceptibility testing
The obvious goal of therapy in infectious disease
is to eradicate, or at least suppress, the pathogen
responsible for the infection. In serious infections,
this goal is achieved through the use of an antimicro-
bial agent. If the pathogen belongs to a species for
which the pattern of drug susceptibility is essentially
invariant, laboratory identification of the pathogen
constitutes adequate information on which to base
drug selection. If there is clinically significant
variability in the pattern of drug susceptibility of the
species, it is desirable to determine the susceptibili-
ties of the organism isolated from the patient so that
the most appropriate therapeutic agent can be
provided. One way to do this is empirically, by
administering the drug, or drug combination, most
likely to be effective and seeing if it works. If it
does, fine; if it doesn’t, the organism can be
assumed to have low susceptibility to that drug, or
that combination of drugs, and another can be tried,
either alone or in combination with the initial
drug(s). It must be noted that, even when effective
antimicrobial agents are used, the clinical signs of
infection may persist for a while. For example, a
patient with uncomplicated cystitis may have her
dysuria disappear within a few hours of the first dose
of an effective antibiotic but a patient with
pyelonephritis may continue to have fever and flank
pain as long as 2 days after the start of appropriate
antibiotic therapy.
Tissue Injury
9-17
0
2
4
6
8
10
12
Relative concentration
HBsAg
HBeAg
0
2
4
6
8
10
12
Time after exposure (months)
Relative concentration
anti-HBs
anti-HBe
anti-HBc
0
2
4
6
8
10
12
Relative concentration
HBV DNA
and
DNA polymerase
Figure 9.4
The diagnostic windows for markers of acute
hepatitis B infection. The top graph shows the window for
viral HBV DNA and DNA polymerase, the middle graph
shows the windows for viral antigens, and the bottom graph
shows the window for HBV-specific antibodies.


