identified by studying a number of related individu-
als both with and without the disease. Conducting
family studies is at best difficult and is sometimes
impossible (Korf 1996).
Northern blot hybridization.
Genetic abnor-
malities that result in abnormally sized mRNA can
be demonstrated in a manner similar to that of the
Southern blot technique with the exception that
enzymatic digestion is not required. mRNA is
extracted from a tissue in which the gene is
expressed. It is then separated according to length
by gel electrophoresis and transferred to a nitrocellu-
lose filter by blotting. Labeled DNA probes hybrid-
ize to the sequence of interest marking the location
of the mRNA.
Under carefully standardized and controlled
conditions, the intensity of the hybridized label is
proportional to the level of expression of the gene so
this technique can be used to quantified transcrip-
tional activity. This can be helpful in the evaluation
of diseases in which the mutation resides in the
regulatory DNA rather than the coding DNA.
Genetic disorders of metabolism
The genetic disorders of metabolism arise from
abnormalities of membrane transport proteins and of
the enzymes that catalyze the anabolic and catabolic
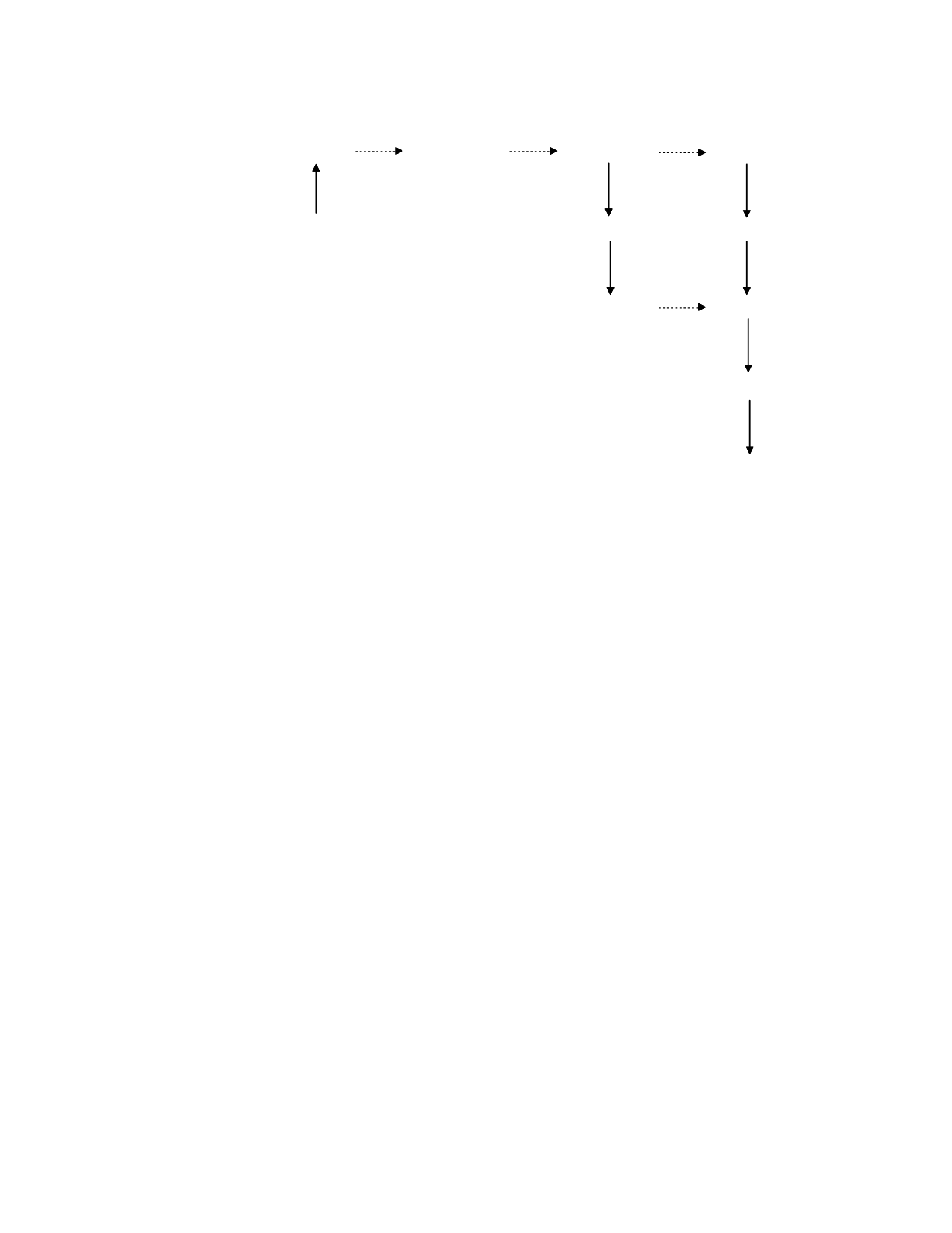
reactions of intermediate metabolism. The general
model of metabolic fluxes illustrated in Figure 10.4
reveals the numerous locations at which such a
genetic defect can appear. There may be impaired
transport of a precursor substance into the anabolic
tissue (site 1 in the Figure), of end product into its
catabolic tissue (site 5), or of catabolites through the
excretory pathway (sites 7 and 8). Disordered
metabolic transformations can occur in the anabolic
tissue (sites 2, 3, and 4) or in the catabolic tissue
(site 6).
As a rule, the presence of a metabolic defect
results in the decreased appearance of substance in
the metabolic pathway distal to the defect and the
accumulation of substances proximal to the defect,
especially of the substance immediately proximal.
Table 10.5 gives a scheme for substance accumula-
tion based upon the site and mechanism of the
metabolic defect. Note that when there is no reflux
of accumulated substance out of the cell, accumula-
tion is strictly intracellular and can only be evaluated
by examination of involved tissues. When reflux
does occur, substance accumulates in the body fluids
as well as intracellularly. Substance accumulation
can then be detected and quantified by the measure-
ment of the substance in readily obtained and
analyzed specimens such as plasma and urine.
When there is a defect in a biosynthetic pathway
(Figure 10.4, sites 2 and 3), the synthesis of alterna-
tive end products may be increased due to shunting
of accumulated precursor or intermediate substances
into alternative metabolic pathways.
The pattern of end product deficiency, interme-
diate product accumulation, and alternative end
product appearance is often highly diagnostic for the
underlying defect. Congenital adrenal hyperplasia,
serves as an interesting example (Miller 1997). The
Genetic Disease
10-7
ANABOLIC
TISSUE
precursor
intermediates
end product
catabolites
BODY
FLUIDS
precursor
end product
catabolites
CATABOLIC
TISSUE
end product
catabolites
excretion
7
1
2
3
4
8
6
5
EXCRETORY
TISSUE
Figure 10.4
A model of metabolic fluxes. Numbers mark potential sites of genetic defects.


