1983). The clearance rate is calculated using the
formula,
organ clearance rate
=
amount administered
C
1
ln
{
C
1
/
C
2
}
$
where C
1
is the plasma substance concentration
immediately following administration and C
2
is the
plasma substance concentration of the second speci-
men, drawn at time,
τ
.
If the substance is administered orally, by short
intravenous infusion, or if it has a multiexponential
plasma clearance curve, multiple specimens will be
needed. The number and timing of the samples will
vary considerably from substance to substance so the
appropriate literature should be consulted as an aid
in the design of the sampling schedule and the calcu-
lation of the area under the plasma clearance curve.
In clinical practice, clearance studies often rely
upon a single concentration determination. In such
studies the actual clearance rate is not calculated but,
rather, the extent of substance removal, as indicated
by the plasma concentration of the substance at a set
time following the administration of the substance, is
measured (Figure 7.5). This is a less accurate way
to conduct a clearance study because of the variabil-
ity in plasma substance concentrations that results
from interindividual variability in the volume of
distribution and rate of absorption of the marker
substance. Even if the sampling time for a
one-sample clearance study can be set at a time that
results in little measurement variability for a particu-
lar clearance rate, that time cannot be well suited for
measuring the clearance of substance in patients with
different clearance rates. In particular, for patients
who have a clearance rate less than the one for
which the study performs well, the specified
sampling time will fall earlier in the plasma clear-
ance of the substance when the effects of variability
in the volume of distribution or in the rate of
substance absorption are larger.
ABSORPTION
Absorption is the uptake of a substance by an
organ that conveys that substance to or from the
external environment. Of particular concern to the
clinician are the absorption of oxygen by the lungs,
the absorption of nutrients by the gastrointestinal
tract, and the reabsorption by the renal tubules of
substances filtered at the glomerulus.
Direct measurement of absorptive function is
possible and is frequently employed; the rate or
amount of a substance entering an organ of absorp-
tion can be determined by sampling the input
material and the rate or amount of substance leaving
the organ can be ascertained by sampling the output
of the organ. For instance, the tubular reabsorption
of sodium in the kidney can be quantified by calcu-
lating the rate of sodium input into the tubules
(computed as the product of the plasma sodium
concentration and the glomerular filtration rate) and
by measuring the rate of sodium excretion in the
urine (computed as the product of the urine sodium
concentration and the urine flow rate). Dividing the
rate of excretion by the rate of input yields the
fraction of sodium excreted. One minus that fraction
is the fraction of sodium reabsorbed.
Indirect measurement of absorptive function is
also possible. One approach is to use the
Organ Function
7-4
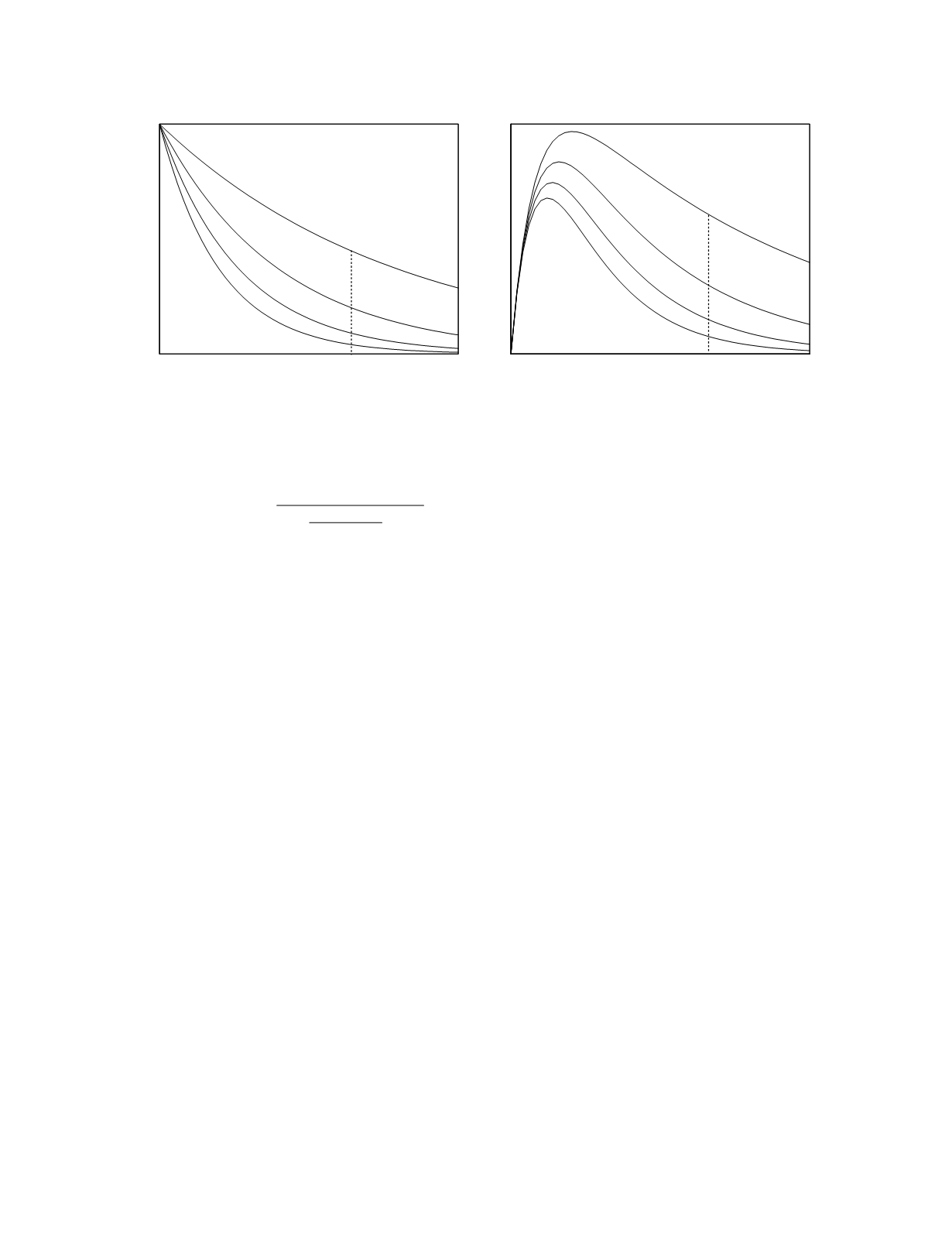
Time
Plasma concentration
Time
Plasma concentration
sampling
time
sampling
time
Figure 7.5
Plasma disposition curves for an exogenous substance given by bolus injection (left graph) and by oral admini-
stration (right graph). For each mode of administration, the disposition curves for four different clearance rates are shown.


