the reliability of the result of the study. Additional
problems with ex vivo studies include variability in
the tumor cell sampling process due to intra-tumoral
cancer cell heterogeneity and loss of the stromal and
vascular setting that defines the tumor's microenvi-
ronment in the patient. Despite these obstacles, a
number of
ex vivo
drug sensitivity assays have been
developed and new ones continue to be developed
(Bellamy 1992, Cree and Kurbacher 1997) although,
to date, none of the assays has been shown to be
reliable enough for clinical use.
Monitoring
Clinical monitoring of a cancer patient consists
of monitoring the patient’s tumor and monitoring the
physiologic status of the patient. Tumor monitoring
may be undertaken to evaluate the response to
therapy, to detect the recurrence of a cancer follow-
ing successful therapy, or to assess the progress of
an established tumor. Monitoring is accomplished
primarily by clinical examination, imaging studies,
and, for some tumor types, by serial measurement of
the plasma concentration of a marker substance. In
leukemias, monitoring relies on serial counts of
cancer cells in blood. A number of techniques are
currently being developed for the detection of micro-
metastatic carcinoma cells in blood and bone marrow
and of cancer cell DNA in plasma (Pantel and von
Knebel Doeberitz 2000). Laboratory studies based
on these techniques will allow much greater analytic
sensitivity in the monitoring of tumors.
Conventional treatment has aimed for eradication
of cancer but newer approaches may produce growth
control rather than cell death. Therapy directed at
suppressing tumor growth may be expected to stabi-
lize the plasma concentration of a tumor marker. If
the intent of therapy is to reduce the number of
cancer cells, with the hope of totally eliminating the
cancerous clone, the plasma concentration of a
tumor marker will be expected to decline over time.
The rapidity of the decline will be determined by the
rate of cell loss in the tumor (in response to the
Cancer
11-17
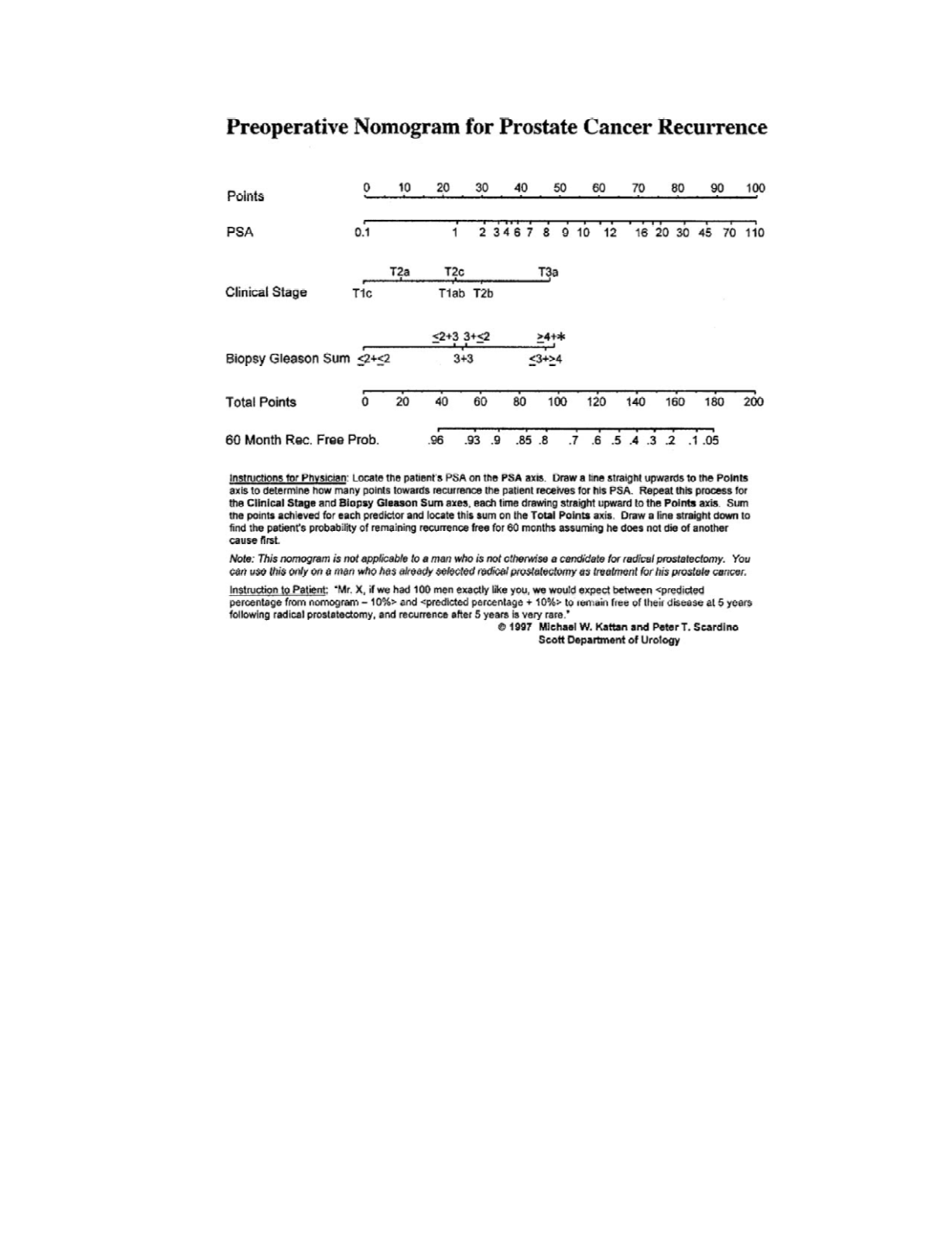
Figure 11.8
Nomogram for calculating the probability of prostate cancer recurrence within 5 years following radical
prostatectomy. Reprinted from Kattan MW, Eastham JA, Stapleton AMF, Wheeler TM, and Scarpino PT. 1998. A preopera-
tive nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst 90:766.


